Original text from Shunichi Ono 15.05.2012 http://onodekita.sblo.jp/article/55872777.html
About papillary thyroid cancer, I only had knowledge from the national exam of medical practitioners. I reread my old textbook.
About the papillary thyroid cancer
Papillary Thyroid cancer is most common among thyroid cancer, and it appears most commonly in women from 30 to 50 years old.
Cancers in youth often carry a poor prognosis, but this cancer has an excellent prognosis, and ten year survival rate is more than 80%.
Almost all thyroid cancer caused by exposure to radiation is papillary thyroid cancer, so that it was also most commonly observed after The Chernobyl Disaster in 1986. Furthermore, it is pointed out that providing a neck irradiation treatment for children under 10 year old increases the risk of this cancer.
This cancer is often caught when firm nodular goiter is discovered, and it metastasizes mainly to lymphogenous. In some cases, it already metastasizes to cervical lymph nodes at the initial visit, or to other organs such as lung or bone, but because of its slow growth, prognosis is not so bad. It is not likely to infiltrate, however, in a case of advanced cancer, recurrent nerve paralysis or difficulty swallowing by infiltration to throat can occur.
Diagnosis
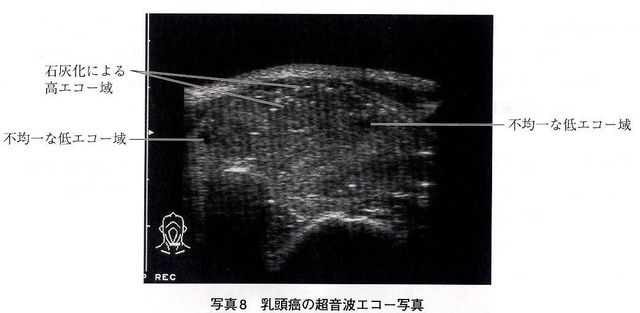
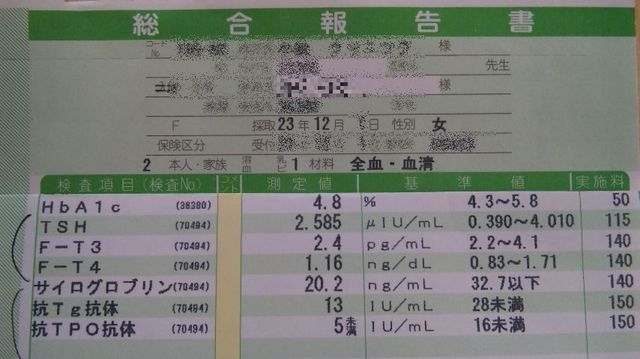
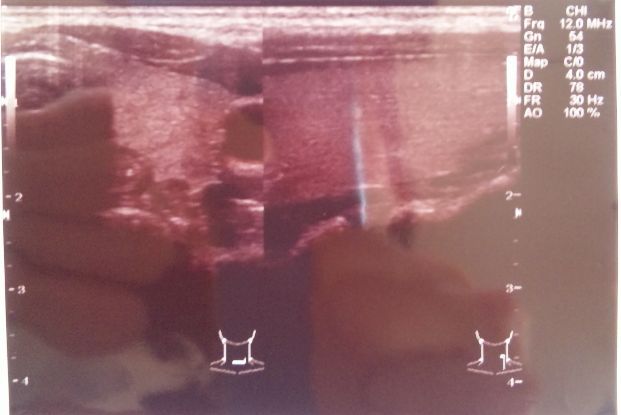
Papillary Thyroid cancer and Follicular cancer, a differentiated cancer of the thyroid, don't produce hormone but behave like they do, which causes thyroglobulin level in the blood to rise. However, thyroglobulin level also rises with many other diseases, so it doesn't assist in diagnoses so much. Psammoma Body can be found by soft radiograph of neck, which used to be a popular diagnoses. However, with the progress of the other diagnostic imaging technique, it is rarely used today. Most common diagnoses today is Ultrasonographic examination. A mass can be found by Ultrasonography, Internal echo of a mass is heterogeneous and low, thus comes out black with its irregular margins. Ultrasonic wave can not go through a mass, so that a backward echo becomes weak or disappears. Also, it recognizes a scattered high echo zone under the hood, which is formed when it calcifies.
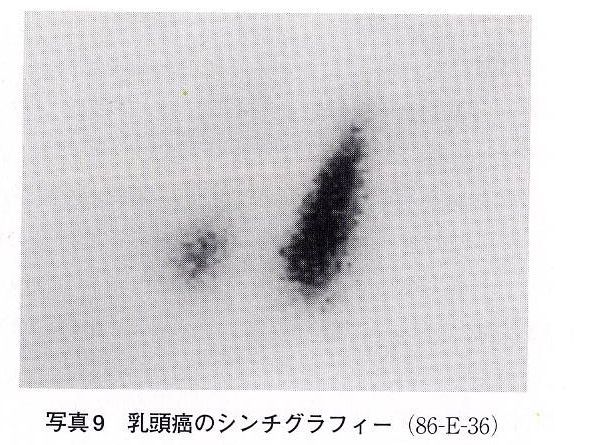
As this cancer doesn't produce hormones, Thyroid Scintigraphy using 123l or 99mTc is not given permission to be captured so it becomes "cold". However, when it metastasizes to a lung or a bone, it is captured at these region and becomes "hot". In the case of Scintigraphy using 201Tl, retaining time in a mass is longer so that it becomes "hot".
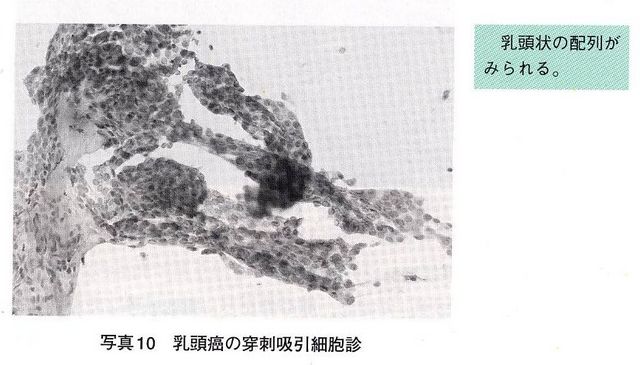
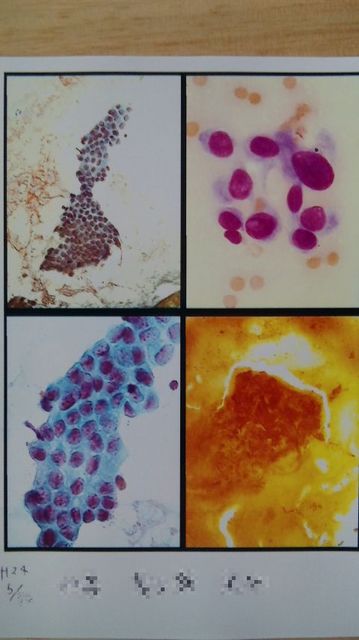
Big amount of tumor cells that form a colony can be collected by Fine-needle aspiration cytology (FNAC), and cell colony has either papillary or sheet-like arrangement. A frosted glass-like nucleus lies inside of a cell, and a nucleolus that is located on its margin, which looks oculate, is clearly visible. In other cases, cytoplasm invaginates into a nucleus and forms cleaves, so that it looks like an inclusion body. (Intranuclear cytoplasm inclusion body)
Treatment
It is treated by surgically removing, however, this cancer has good prognosis, so there is a discussion when to remove. The thyroid removing requires some attention not to damage a nervus laryngeus recurrens or nervus laryngeus superior. In addition, it is necessary to pay attention to hypocalcemia resulting from a accessory thyroid removing.
Tumor cell of this cancer is considered to develop to THS-dependent. In some cases, synthetic T4 administration is given in dose sufficient to inhibit THS for shrinking tumor. (This treatment is controversial and not established)
If a tumor develops metastasis into a lung or a bone, Thyroid Sintigraphy using 131l is applied after a complete removal of thyroid. If it is captured successfully, get rid of a tumor by a big amount of 131l administration. Not 123l that has a small radiation exposure but 131l that releases intense beta ray is used. Be sure to remove thyroid completely in advance, otherwise 131l is taken into thyroid, which cuts in half the effect of the treatment.
Those are basic knowledge that medical students should know.
I got contacted by a woman in her early 30s who evacuated from Fukushima (Kôriyama) to the west Japan. She was diagnosed with papillary thyroid cancer and is going to have an operation. She gave me a permission to introduce her note on this blog. We can't determine that her cancer is caused by the accident, but we should certainly take it as a warning sign.
Where she was / What she did after the accident
March 11 - 15, 2011
In Kôriyama City until 15th noon
She wore a normal mask when going out. N95 Mask for radioprotection wasn't available at that time. Water was cut off, so she queued for a bath or fetching water. She kept windows closed. but didn't seal them up.
Her place is on the ground floor in a condominium building. On 14th, she took 10ml of Isodine. On 15th, plume covered all over Tokyo and the neighboring area. She left Kôriyama in the afternoon, as if following the plume, and arrived at Numazu(Shizuoka Prefecture)in a rain. As the highway was closed to traffic, she took the local way and the whole trip took as much as 15 hours.
March 16 - April 4
In Numazu
She lived normally. When the second radioactive plume arrived on 21st, she did not go out as it was raining.
April 5 - 23
She stayed in Inawashiro and Nasu, because her place in Fukushima was not in an habitable state and also Ko-riyama measured radiation rate as much as 2μSV.
April 24 - September
In Aizuwakamatsu
As she should / wanted to continue her work, she moved to Aizu, where contamination is much less. Radiation level there was about 0.14μ then. However, she drove to Tochigi or Senday everyday for her work. Though she never entered within 80KM area from the plant, she often passed by Ko-riyama or Fukushima.
September - January
Moved to Numazu
January --
Moved to somewhere in west Japan (west to Osaka)
She has been trying to avoid contaminated foods and water.
She underwent urine testing at RIKEN on 21 and 22 February 2012. Neither Iodine or Cesium was detected, which detection limit is 0.073.
July 2011
She went to a hospital in Aizu.
She had a throat ache, sputum and diarrhea, she lost weight and felt sick and tired, so she went to checkup in a hospital. a 5-mm tumor was found by an ultrasonic diagnosis. She hadn't discovered a lump herself. She also had a cytologic diagnosis. The amount of cells was insufficient, so the result came out as "indeterminable", but then the doctor told her there was no problem. When she expressed her worries about radiation, the doctor just laughed it away.
December 2011
She went to a clinic in Shizuoka
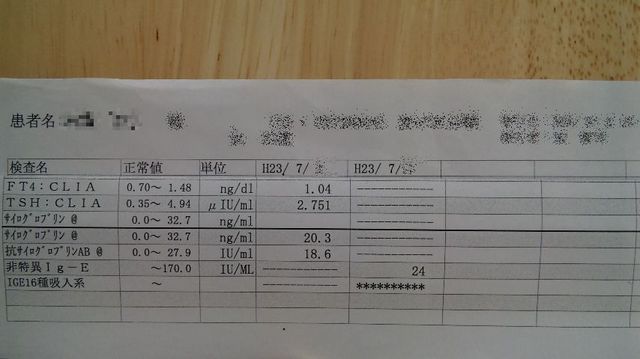
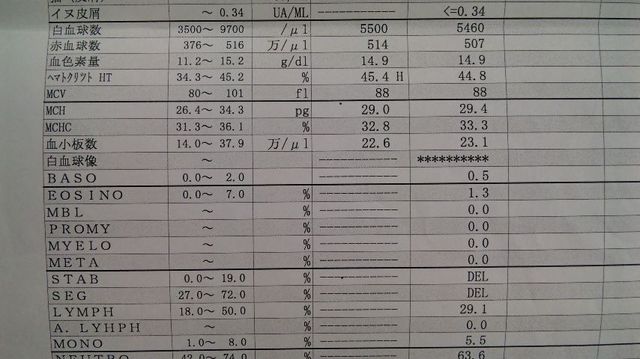
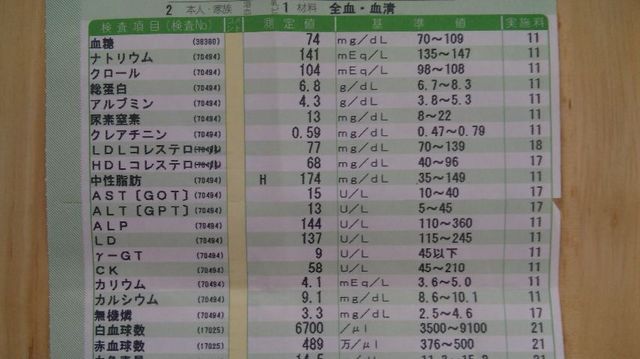
She brought a referral form, and had an ultrasonic diagnosis and blood test.
The tumor has grown to 6 mm, but we can't receive a cytological diagnosis until it grows more than 7 mm. No abnormality was found by blood test. Doctor said to her that one or two examination per year is enough.
April 2012
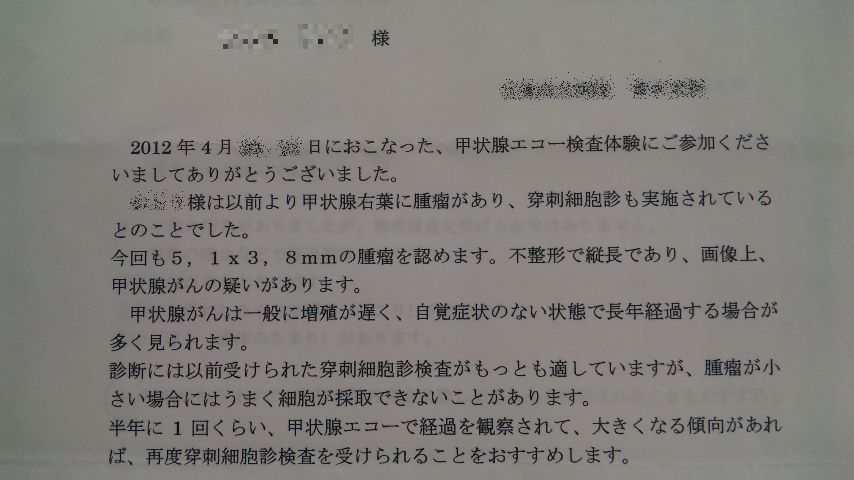
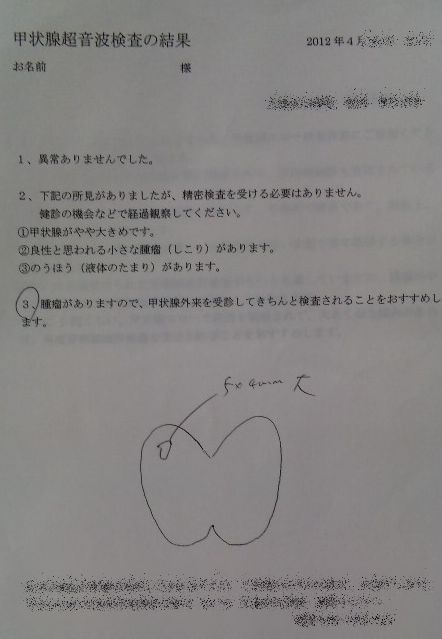
A group of evacuee including her organized an event, and offered a free ultrasonic diagnosis. she knew she had a lump, but as it was free, she went to have another test. A doctor explained to her that she got an irregular shape of lump, which are usually malignant, and recommended her a periodic examination. It was the first time she heard about the shape of lump.
April 2012
She had a colored ultrasonic diagnosis, blood test, cytological diagnosis, electrocardiogram and urinary examination at another clinic. 2 weeks later, she went to discuss her results with her doctor. "One doesn't die of thyroid cancer" said the doctor at first.
She has had kind of predicted it from the result of ultrasonic diagnosis, so she was pretty prepared then. Her pulse was only 50, and she got an underactive thyroid function. She wondered what was a cause of disease, and there were many she could think of, but among them the most convincing to her was the stress of work and changes of her life.
May 2nd
She went to the clinic again. She had another cytological diagnosis to verify the result from the last diagnosis. According to the doctor, the result could be affirmed by staining the sample cells. She went to the clinic 2 weeks later to get informed of the diagnosis.
May 3rd
Third time to the clinic again.
She had an uneasy feeling when she received a phone call from the clinic 4 days after the diagnosis, giving her an appointment to discuss her results, which was supposed to take 2 weeks. She was diagnosed with papillary thyroid cancer.
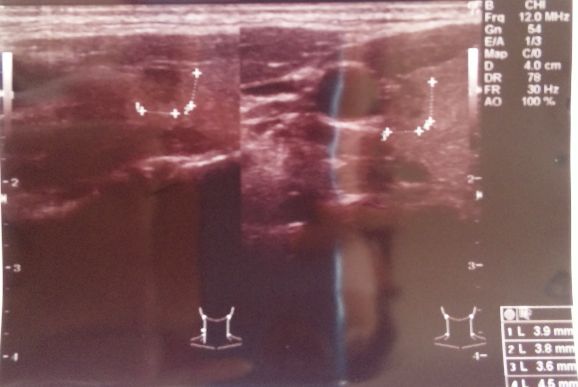
The 6 mm tumor appears on the right side of thyroid.
The doctor told her about the diagnosis while showing the image of cytological diagnosis. Doctors with less experiences could have determined the tumor as benign, but her doctor was the one who specialized in treating persons affected by radiation, and did some study in Chernobyl as well. He also understood that she was from Fukushima, and radiation could give a health damage.
I quoted her memo with only a few edit (for protecting privacy). This is all what i got, so please understand that I'm not able to answer any further questions.
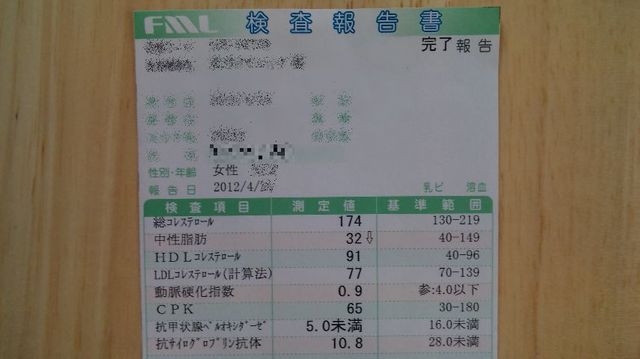
However, as it was written, she had 10ml of Isodine after the accident, left Ko-riyama quite quickly and also no abnormality in her thyroglobulin level is found. Considering all those facts, I should not prejudge but I can't help expecting that we are going to have a catastrophic health hazard caused by the accident.
As for the Thyroid cancer, Dr. Shunich Yamashita, who calls himself as an leading authority, gives this lecture introduced below. According to him, thyroid cancer won't increase for the 3 years after the accident. Also, Thyroid cancer Association, an association that Dr. Yamashita chairs the director, issues a proclamation like this:

Don't we need to rethink this situation?
0 件のコメント:
コメントを投稿